 Overview
OverviewA hammer toe can be defined as a condition that causes your toe to bend downward instead of pointing forward. While it can occur on any toe on your foot, it usually affects the second or third toe. If your baby toe curls instead of buckling, it is also considered a hammer toe. There are two types of hammer toes. If your toes still can move around at the joint, then it is considered a flexible hammer toe. It is a milder form of the condition and there are more treatment options. The other type is called a rigid hammertoes, which occurs when the tendons in your toe become so rigid that they push your toe joint out of alignment, and it cannot move at all. Typically, you will need surgery to fix it.
Causes
Hammertoe commonly develops because of structural changes that take place over time in the muscles and tendons that bend the toes. People with certain medical conditions, such as diabetes, are at risk for developing hammertoe. It can be an inherited condition for some people. Other causes include trauma and wearing shoes that are too tight, narrow, or have high heels. The toe next to the big toe (second toe) is most frequently affected by hammertoe.
 Symptoms
SymptomsThe symptoms of hammertoe are progressive, meaning that they get worse over time. Hammertoe causes the middle joint on the second, third, fourth, or fifth toes to bend. The affected toe may be painful or irritated, especially when you wear shoes. Areas of thickened skin (corns) may develop between, on top of, or at the end of your toes. Thickened skin (calluses) may also appear on the bottom of your toe or the ball of your foot. It may be difficult to find a pair of shoes that is comfortable to wear.
Diagnosis
Some questions your doctor may ask of you include, when did you first begin having foot problems? How much pain are your feet or toes causing you? Where is the pain located? What, if anything, seems to improve your symptoms? What, if anything, appears to worsen your symptoms? What kind of shoes do you normally wear? Your doctor can diagnose hammertoe or mallet toe by examining your foot. Your doctor may also order X-rays to further evaluate the bones and joints of your feet and toes.
Non Surgical Treatment
Symptomatic treatment of hammertoes consists of such things as open toed shoes or hammertoe pads. There are over the counter corn removers for temporally reducing the painful callous often seen with the hammertoe. These medications must be used with caution. They are a mild acid that burns the callous off. These medications should never Hammer toes be used for corns or callouses between the toes. Persons with diabetes or bad circulation should never use these products.
Surgical Treatment
Surgery to correct for a hammertoe may be performed as an outpatient procedure at a hospital, surgery center, or in the office of your podiatrist. There are multiple procedures that can be used depending on your individual foot structure and whether the deformity is flexible or rigid. There may be a surgical cut in the bone to get rid of an exostosis, or a joint may be completely removed to allow the toe to lay straight.


5I1dimw~~60_35.JPG)

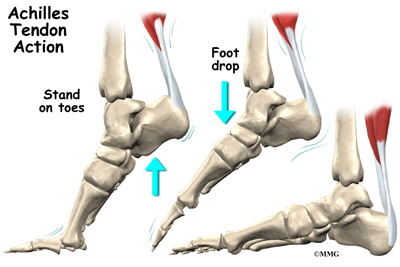
 The Achilles tendon is the largest tendon in the body. Tendons are long, tough cords of tissue that connect muscle to bone. The Achilles tendon is located in the back of the foot and connects your heel bone to your calf muscle. It helps you to walk, run and jump. The Achilles tendon is able to endure stress, but sometimes injury can occur to the tendon when overly stressed. Overuse of the Achilles tendon may cause the tendon to swell, become irritated, inflamed and cause pain. This is Achilles tendinitis. It is a common sports injury related to running, but can happen to anyone who puts a lot of stress on their feet (e.g.: basketball players and dancers). If you do not get treatment for Achilles tendinitis, the problem can become chronic and make it difficult for you to walk.
The Achilles tendon is the largest tendon in the body. Tendons are long, tough cords of tissue that connect muscle to bone. The Achilles tendon is located in the back of the foot and connects your heel bone to your calf muscle. It helps you to walk, run and jump. The Achilles tendon is able to endure stress, but sometimes injury can occur to the tendon when overly stressed. Overuse of the Achilles tendon may cause the tendon to swell, become irritated, inflamed and cause pain. This is Achilles tendinitis. It is a common sports injury related to running, but can happen to anyone who puts a lot of stress on their feet (e.g.: basketball players and dancers). If you do not get treatment for Achilles tendinitis, the problem can become chronic and make it difficult for you to walk.



 A tendon is a band of connective tissue that anchors muscle to bone. The Achilles tendon is the largest tendon in the body. It attaches the calf muscles to the heel bone (calcaneus) and is very important because it lets you lift your heel when you start to walk. It also helps you to walk, run or stand on tiptoe. Achilles tendonitis is inflammation of the Achilles tendon. In most cases, it is a type of overuse injury and is more common in younger people. Professional and weekend athletes can suffer from Achilles tendonitis, but it is also a common overuse injury in people not involved in sport. Treatment includes rest, non-steroidal anti-inflammatory drugs (NSAIDs), physical therapy and avoiding activities that aggravate the condition.
A tendon is a band of connective tissue that anchors muscle to bone. The Achilles tendon is the largest tendon in the body. It attaches the calf muscles to the heel bone (calcaneus) and is very important because it lets you lift your heel when you start to walk. It also helps you to walk, run or stand on tiptoe. Achilles tendonitis is inflammation of the Achilles tendon. In most cases, it is a type of overuse injury and is more common in younger people. Professional and weekend athletes can suffer from Achilles tendonitis, but it is also a common overuse injury in people not involved in sport. Treatment includes rest, non-steroidal anti-inflammatory drugs (NSAIDs), physical therapy and avoiding activities that aggravate the condition.




 RSS Feed
RSS Feed